Surgeon hails benefits of mini bypass procedure
Pete Myall, Online Editor, Bariatric News
Contrary to common misconceptions, the mini gastric bypass is a “simple, safe and effective” alternative to the more common Roux-en-Y technique, according to a surgeon presenting his initial experience with the operation.
Speaking at January’s British Obesity and Metabolic Surgery Society meeting in Glasgow, Scotland, Mr Michael Van den Bossche, of Spire Southampton Hospital, said that the operation was popular with his patients and “probably” engendered greater weight loss than the conventional technique.
Van den Bossche investigated the mini gastric bypass by comparing the first 52 patients he operated on using the technique with 52 patients who received a Roux-en-Y gastric bypass.
After 12 months, the mini gastric bypass group had lost an average of 75% of their excess weight, significantly higher than the Roux-en-Y group who had lost 63%. The mean BMI of the Roux-en-Y group dropped from 48.84 to 33.93, while the mini gastric bypass group dropped from 48.4 to 31.6.
The two groups experienced similar rates of comorbidity resolution, including for type 2 diabetes, hypertension, and functional improvement.
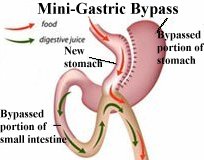
Van den Bossche said that his results showed that concerns about the mini gastric bypass leading to unacceptable complications, particularly bile reflux and oesophageal cancer, were ill-founded. “A lot of people thought the mini gastric bypass was exactly the same as the Mason bypass – a bowel loop on a stomach pouch,” he told Bariatric News. “But the Mason-Ito bypass was a very short proximal pouch with a horizontal bisection line, and then you had bile exposed really close to the oesophagus, giving terrible reflux.”
He said that the mini gastric bypass had a much longer stomach pouch than the Mason bypass – effectively forming a sleeve, with the bowel loop connected to the bottom – which means that bile is kept away from the oesophagus.
“You can have a bit of bile reflux – there will be a small, small percentage,” he said. “But you also get Roux-en-Y patients with reflux.”
Only one of Van den Bossche’s patients suffered unacceptable levels of bile reflux; this patient was one of three out of the 52 who required a conversion to Roux-en-Y gastric bypass. The overall reoperation rate in the mini gastric bypass group was 5.8%, which Van den Bossche attributed to the learning curve.
He said that another advantage of the operation was that a surgeon was able to modify an operation if it turned out to be unsatisfactory. “If it goes wrong, the mini gastric bypass still has a lot of options available,” he said. “People with the Roux-en-Y who have weight regain, for instance, it’s a nightmare to do something for them. Very difficult. With a mini gastric bypass you can disconnect the bowel, and then you can make it longer or shorter. With the Roux-en-Y you can’t – all your bridges are burnt, really.”
Tricks and traps
Van den Bossche said that part of the learning process for the operation was identifying and avoiding “tricks and traps” to ensure a successful operation.
“If you’re a Roux-en-Y surgeon, which I was, you tend to make short pouches,” he said. “When you start mini gastric bypass, you start making your pouch too short. It’s counter-intuitive to go that low in the antrum for your first section – you’re not going a fair bit lower than a Roux-en-Y gastric bypass, you’re going a whole lot lower.”
He also noted the importance of avoiding obstructions when creating the anastomosis. “There are different techniques that have been described,” he said, “but that’s something that everyone has to work out for themselves what they’re most comfortable with.”
Introduction
Van den Bossche said he was introduced to the operation by his friend Dr Jacques Himpens, who had himself brought the operation to Belgium. He says he was drawn to it by a number of factors, including its simplicity and the fact that it lowered the risk of late complications, compared to the Roux-en-Y bypass. “When people think of [fusion_builder_container hundred_percent=”yes” overflow=”visible”][fusion_builder_row][fusion_builder_column type=”1_1″ background_position=”left top” background_color=”” border_size=”” border_color=”” border_style=”solid” spacing=”yes” background_image=”” background_repeat=”no-repeat” padding=”” margin_top=”0px” margin_bottom=”0px” class=”” id=”” animation_type=”” animation_speed=”0.3″ animation_direction=”left” hide_on_mobile=”no” center_content=”no” min_height=”none”][Roux-en-Y] complications, they usually think about leaks and bleedings,” he said, “but there are quite a lot of late problems. Quite a bit of bowel obstructions and internal hernias.”
“The mini gastric bypass doesn’t really have that problem. You don’t actually divide the bowel or have a second anastomosis. That looked very, very interesting.”
He said that the simplicity of the operation also meant that it was popular with his patients; he now offers new patients the choice of the Roux-en-Y bypass and the mini bypass, and around 80% pick the latter. “It appeals to them, because you only have one anastomosis and you have a good exit strategy if there is a problem, which you do not have with any other procedure,” he said.
Mr Carl Dorey, one of Van den Bossche’s patients, said that the operation, which helped him drop his BMI from a high of 57 to 27, changed his life. “I had sleep apnoea; joint pains – a couple of times I was on crutches for a few weeks; I had high blood pressure, asthma, I was borderline diabetic. That all totally went within a few months of having surgery.”
“My energy levels are through the roof,” he said. “I’m walking everywhere now – I have a positive attitude. I feel a lot more organised. Before I was just putting things off or forgetting things because of this lethargic feeling.”
[/fusion_builder_column][/fusion_builder_row][/fusion_builder_container]